

Brief history
In 1903, Codivilla A. successfully performed the first limb lengthening procedure by performing osteotomy, followed by continuous stretching and casting. After that, several physicians such as Magnuson and Fasset also performed similar surgeries. However, this type of surgery caused various severe complications and sequelae like skin and nerve damage, tendon tears, pseudarthrosis, incorrect healing due to uncontrolled stretching rate as well as immobilized bone cavity.
In 1913, Louis Ombre’danne attempted to perform femoral osteotomy followed by stretching that created a 4cm cavity. He used an external fixator with 2 nails and reached the stretching rate of 5mm per day. However, the fast stretching rate caused skin necrosis and infection. In addition, the fixator was not firm as it only had 2 nails. After that, many practitioners attempted to improve the fixator to make it more stabilized and improve osteotomy techniques by paying more attention to the periosteum, setting up a waiting time after the osteotomy, etc. Despite the attempts, the risk of severe complications such as pin site infection, skin and nerve damage, nonunion, incorrect healing and joint deformity was still high.
In 1963, Wagner H. performed a limb lengthening procedure using a monolateral external fixator on the diaphysis after removing the hindering periosteum and soft tissues, with the stretching rate of 1.5-3mm per day. After the desired length had been reached, the patient’s bone was compressed with splints and it also received grafting. However, many complications such as infection, poor healing, reoperation, etc. still occured, thus this technique was no longer applied.
In 1951, a Russian professor named Gavriil Abramovich Ilizarov created a ring external fixator to treat bone fracture and assist in leg lengthening procedures. Based on researches from tests on animals, he discovered the principle of distraction osteogenesis and applied it to limb lengthening: Use the osteotomy technique that preserves most of the bone tissue such as periosteum and bone marrow. The cavity should be slowly stretched at the rate of 1mm per day with an elastic external fixator. Compress the stretched limb early and start to do exercise for the joints as soon as possible. The cavity will slowly be filled with new bone. The limb lengthening procedure is successfully performed without bone grafting and with minor soft tissue damage.
By applying external fixation and osteotomy techniques, with the same stretching rate, in 1971, Ilizarov.G.A announced the results of 215 cases of limb lengthening that he performed with the raised length ranging between 3 and 24 cm. There were 20 patients with limb length discrepancy ranging from 9 to 24 cm. There were 19 cases with complications: meralgia paresthetica (4 cases), pin-site inflammation (11 cases) and osteomyelitis (4 cases).

However, it was not until 1981 did Western countries notice Ilizarov’s limb lengthening technique when he was invited to come to Italy to introduce it. Soon after that, the technique was widely spread, applied and developed around the world as a revolutionary breakthrough in limb lengthening.
During the 1990s, with the development of external fixators and the application of Ilizarov’s limb lengthening principle, limb lengthening had produced better results with fewer complications. At the moment, we can divide leg lengthening into 3 types:
- Leg lengthening using standard external fixation.
- Leg lengthening using external fixation and internal fixation (an intramedullary nail with latches or locking splints)
- Leg lengthening using self-stretch intramedullary nailing (we will publish an article on the advantages and disadvantages of self-stretch intramedullary nailing at a later date)
Principle of bone healing
From the researches based on experiments made by Ilizarov.G.A and Aronson J, we can see that the bone healing process in limb lengthening goes through the following stages: waiting, stretching and healing.
- Waiting stage: During the waiting stage, hematomas and inflammatory cells start to infiltrate the bone cavity (lasts for 7-10 days)
- Stretching stage: During the stretching stage, with the stretching rate of 1mm per day, divided to 3-4 times a day, mesenchymal stem cells start to form a collagen sphere and immature vascular vessels. After that, they self-organize in accordance with the stretch direction. There are 5 cellular zones of distraction osteogenesis (Figure 1.1): In the center of the cavity is the fibrous interzone (FIZ) with the width ranging between 4 and 8mm, composed of cylindrical fibroblasts that are lying loosely along the collagen bundles. Next to the fibrous interzone are two zones of primary mineralization front (PMF) that consist of primordial bone tissues that are being mineralized. The microcolumn formation (MCF) lies next to the primary mineralization front and connects to each bone section. This zone consists of microcolumns of mineralizing bone that are parallel to tension applied during distraction and have bottom at the bone section. Surrounded by vascular vessels, these microcolumns do not possess any Havers unit, cartilage cell or osteoclast. During the stretching stage, the fibrous interzone remains a constant width of 4-8mm, while new bone continues growing in the two ends of the bone. After the stretching stage ends, the fibrous interzone is ossified and forms a microcolumn formation zone that fill the cavity.
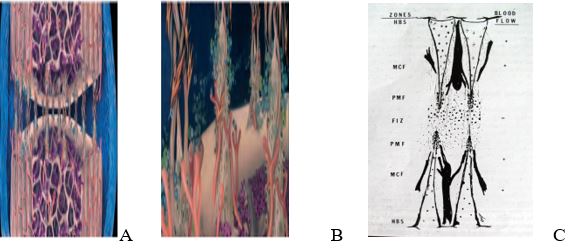
Model of the bone production in the stretch area
A. Figure that illustrates the bone production units that connects the two bone sections.
B. Figure that illustrates a bone production unit.
C. Schematic of the five cellular zones of distraction osteogenesis.
*Source: Al-Aql, Z. S., et al. (2008).
Healing stage: During the healing stage, the newly-formed bone zone grows to form periosteum and bone marrow. Newly-formed bone tissues slowly develops to the structure of normal bones. It usually takes at least a year after removing the fixation for the bone structure to get strong and for the bone marrow to go back to the state before the osteotomy. The stretched bone is strong enough to withstand the forces of compressing, bending and twisting like normal bones.
Assoc. Prof., Ph.D. Le Van Doan